
Report: Spine Disorders

Minimally Invasive Surgery for Adult Spinal Deformity
Research has found that adult spinal deformity (ASD) patients with both sagittal and coronal plane deformities have worse quality of life than patients who are legally blind or quadriparetic.
When a patient’s symptoms persist despite non-operative therapies, surgical correction of ASD can result in significantly improved outcomes.
Open surgical treatment of ASD consists of stripping all the muscles of the dorsal spine and performing osteotomies. “These procedures can be very bloody, typically require an ICU stay, and are associated with significant post-operative pain,” said spine surgeon Khoi Than, MD. “Major complication rates are around 25% and overall complication rates are around 70%.” Minimally invasive surgery (MIS) can accomplish the same correction without these drawbacks.
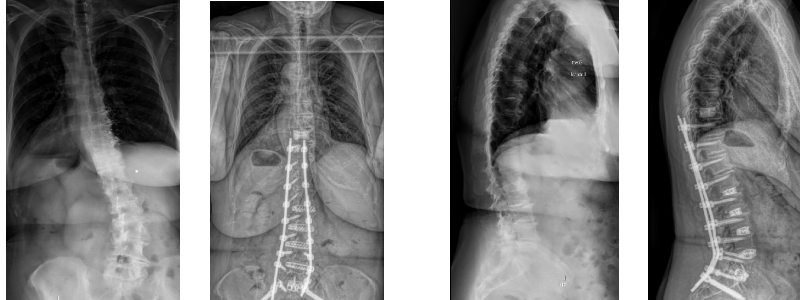
Minimally invasive deformity correction relies on the presence of intact disc spaces, Than explains. By releasing the annulus fibrosus bilaterally across multiple disc spaces, coronal correction is accomplished; by placing appropriately lordotic cages, sagittal correction is accomplished.
A typical MIS deformity procedure consists of an anterior lumbar interbody fusion at L5-S1, minimally invasive lateral lumbar interbody fusion from L1-L5, and pedicle screws placed percutaneously from T10-S2. Stereotaxy can then be used to cut rods to an appropriate length and contour them such that the spine is reduced to the rod. “Such procedures involve minimal blood loss, generally do not require an ICU stay, and (at least anecdotally) are less painful to the patient in the immediate post-operative period,” said Than.
When You Don't Want to Miss a Thing: Awake Spinal Surgery
Awake surgery is an attractive option for patients who are at risk for adverse reaction or long recovery from general anesthesia. The first such surgery at Duke was performed by Muhammad Abd-El-Barr, MD, PhD, in November 2019 and came about when a patient asked if there were alternatives to going under. Since that time, he has completed nearly 100 cases. The benefits of the surgery without general anesthesia include a quicker recovery and discharge, sometimes without ever spending time on the hospital floor.
Abd-El-Barr dubbed the procedure an awake spinal anesthetic robotic lumbar fusion, and it required two crucial pieces: decreased tissue manipulation through robotics and advanced anesthesia methods. He collaborated with Duke anesthesiologist Jeffrey Gadsden, MD, on the latter. The pain management plan relied on regional anesthesia and erector spinae plan (ESP) nerve block, which had the added benefit of keeping the patient comfortable for several days following surgery.

Turning Up the Volumes on ACDF
Michael Haglund, MD, PhD, MACM, has completed nearly 8,000 anterior cervical discectomy and fusion (ACDF) cases in his career, averaging around 375 each year.
It’s this kind of volume that has led to consistently low complication rates and has made his practice a draw for patients across the country.
“The experience of performing 8,000 procedures leads to operations that are efficient and brief, resulting in high patient satisfaction scores and excellent outcomes,” said Haglund.
The team also embraces new technology, such as smaller and thinner plates and nanotech cages, and minimally invasive techniques to improve the effectiveness of fusions.
“With every case, our goal is to continually improve,” said Haglund. “I approach each procedure like a Formula 1 pit crew, breaking it down into smaller components to identify opportunities for better and safer execution.”
Getting Personal: Patient-Specific Spine Surgery
Duke spine surgeons are using the application of nerve segmentation using magnetic resonance imaging (MRI) /computed tomography (CT) fusion to determine the safest, last traumatic method of performing percutaneous lumbar fusions.
“We can know, preoperatively, the exact dimensions of neural and bony anatomy,” said Muhammad Abd-El-Barr, MD, PhD. “We can then design pin-point trajectories that allow us to make more room for your nerves and stabilize the bones with almost no blood loss and tissue damage."
Abd-El-Barr and others are collaborating with colleagues in Duke Neuroradiology to get sub-millimeter under-standing of the critical structures in the back. “Our work has shown that we can design specific surgeries for each patient to ensure the safest outcomes and best results,” he said. “Currently, we are manually doing this work, but we hope that this work will be the foundation of using complicated computer algorithms such as machine learn-ing to do the planning and execution of these surgeries even more safely and efficiently.”
Vertebral Body Shortening for Recurrent Tethered Cord
For patients with spina bifida who have tethered cord syndrome, vertebral body shortening is an option that avoids the complication risk associated with revision detethering.
Deb Bhowmick, MD, who specializes in the technique, explains that surgery to release a tethered cord is effective, but the cord can retether, and the surgery can be performed a very limited number of times due to the high risk of injury. “So the patient is left with only pain relief, as they slowly lose the ability to walk,” he said. A solution is shortening the vertebral column by removing a third to half of a vertebra and compressing the spine. “Unlike detethering, spinal shortening is one and done,” said Bhowmick. The procedure is not new, but the tools and technology have advanced greatly in recent years.
Bhowmick estimates he is one of about a half-dozen surgeons who offer this technique. Therefore, patients will travel many miles for access. He and other surgeons offering the procedure have recently formed a consortium to discuss standards and risk reduction.
RESEARCH HIGHLIGHTS
Best Practices in Spine Surgery
Duke is the host site for the ACS Spine Collaborative, a group of 17 hospitals throughout the United States and Canada who abstract CPT-eligible procedure-targeted spine cases in National Surgery Quality Improvement Program. Spine surgeon Oren Gottfried, MD, leads the group.
The goals for the collaborative are to:
- Encourage quality improvement initiatives with engagement of spine surgeons, surgeon champions, and surgical clinical reviewers
- Reduce variation among hospitals and surgeons
- Provide a forum to share and disseminate best practices
Using Predictive Analytics to Improve Outcomes
A new machine learning tool that assesses surgical risk— dubbed Pythia — helps amplify the expertise of Duke providers in predicting postoperative outcomes for different types of high-risk surgeries. The tool was developed by the Duke Institute for Health Innovation.
“This tool draws patient data directly from the electronic health record so we can have complex, real-time data at the point of care,” said Oren Gottfried, MD, Duke spine surgeon. “It can assess a comprehensive set of data points from more than 100,000 patients treated at Duke without any effort on the part of the surgeon.”
The risk calculator is more localized compared to models like the National Surgical Quality Improvement Program risk model, as Pythia is built exclusively on Duke’s own patient population.
Duke spine surgeons are using Pythia’s predictive analytics to help determine if patient’s health could be optimized before surgery, to help select patients for preoperative geriatric or anesthesia consultation and treatment, and to assess if the patient is better suited for a less invasive surgery or nonoperative treatment.
All Chapters
Home / Brain Tumor / Epilepsy / Cerebrovascular & Skull Base / Pediatric / Chronic Pain / Trauma / Movement Disorders / Brain & Spine Metastasis / Spine / Global / Residency / Top Papers